
Are Breast Implants Worth the Trouble, or the Risk?
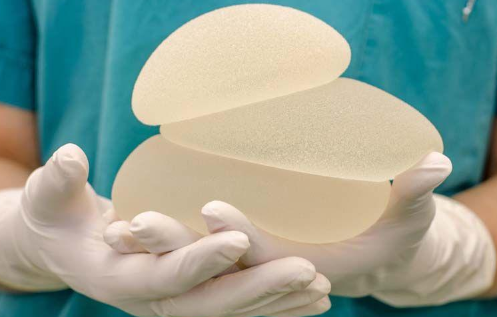
A healthy body image leads to better sexual health, but are breast implants worth the confidence boost? There are several options on the market for breast implants these days; silicone or saline, textured or smooth,… Read More »